MCI Week
for additional information contact your EMS Duty Officer

PROCEDURE
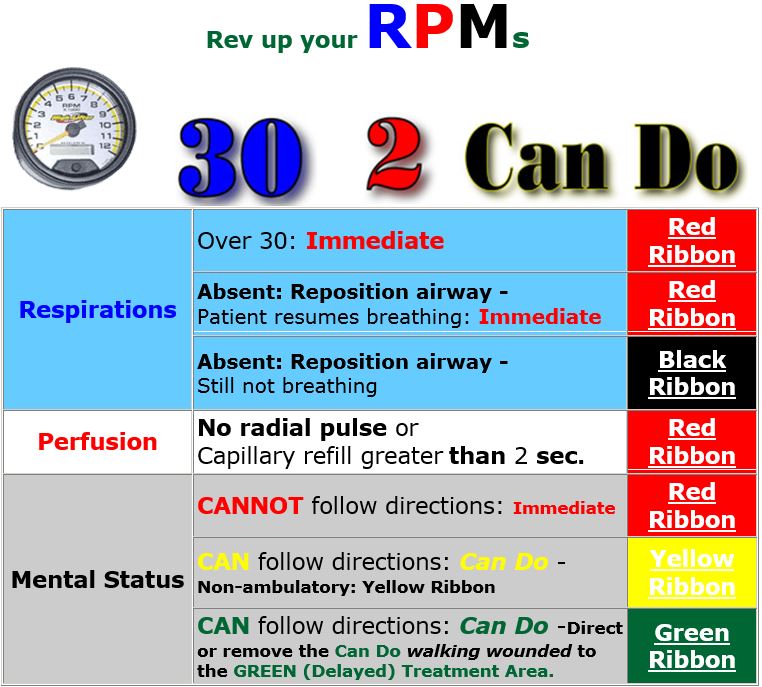
As soon as you recognize that there are more patients than responding units can transport, initiate the Incident Command System, establish an Incident Commander, and begin initial START triage.
If the victims are in multiple vehicles or dispersed over a relatively large area, attach the appropriate ribbon to the patient's wrist (or the ankle if the wrist is unavailable due to entrapment or injury) using START triage criteria.
If the victims are confined to a relatively small area, such as a bus or rail car, consider using ribbons AND tags during initial triage. Do not fill out the tag at this time, simply attach it to the ribbon, remove one of the 6 barcode labels, and stick the barcode label to the seat where the patient is sitting or the floor/ground area where the patient lay. This is of invaluable importance in crash reconstruction and is especially important in incidents involving public transportation and/or fatalities.
Green ribbon (walking wounded or those denying injury) should be removed to a designated place away from the areas where patient extrication or on-scene care are performed. Once all victims have been START triaged, the incident commander can call for appropriate additional units and establish treatment areas for red and yellow ribbon patients awaiting transport.
The fewer people who are involved in the START triage, the better and more accurate the triage process will be. A person who is triaging 10 patients at a given incident has a far clearer view of the 'big picture' than the rescuer triaging only 2 patients. Once START triage has been completed, designated triage personnel should reassess all patients to confirm the findings of the START triage or upgrade/downgrade the victims's priority.
MCFRS MCI Significant Incidents: Presented as option for station officers to engage shift personnel in a tabletop discussion. Review the MCI Significant Incidents as a shift. Identify the common themes for things done well and areas for improvement
MCFRS MCI Significant Incidents (these reports are password protected)
- River Road
- Southlawn Lane
- Dulles Airport
- New Hampshire Ave & Tracy Dr.
- Georgia Ave & Sligo Ave
- Excaliber Ln and Norwood Rd
- Woodfield Rd
- Magruder High School
- Viers Mill Rd
START Triage Powerpoint
TRIAGE Review
Triage Reference Cards (pdf file)
MCI PUBLICATIONS:
Option for Battalion Chiefs to engage station officers, face-to-face or via e-mail with dialog that pertains to each publication
San Bernardino Active Shooter Incident 
J EMS: MCI Efficiency It Takes More than Triage Tags to Run an MCI
Here are five (5) steps you can take to help prevent a negligence claim against you or your agency based on your conduct at an MCI:
Are you prepared to handle a variety of "MCI magnifiers"? Lessons learned from Los Angeles County Fire Dept.'s MCI.
BLANK ROW
Pre Training Survey
Pre-Training Survey
MCI Drill for Unit & Battalion Chief Officers
Active Assailant 
MCI Week Battalion Based Remote Training Scenarios
These training scenarios have been developed to assist the Battalion Chiefs conduct MCI readiness training with their unit officers.
There are two scenarios that have been developed – one active assailant (scenario 1) and one carbon monoxide poisoning (scenario 2). The scenarios are tailored so that the patients can be moved from the scene with the five (5) transport units that respond on an EMS task force.
During these training sessions, the Battalion Chief will be the scenario moderator. These training scenarios were developed with intent that the scenario moderator and unit officers will be at their home station, at a computer terminal, with a radio available. If you wish to have the unit officers assembled at one location, the documents will need to be printed out prior to beginning the training.
Included in the scenarios are interaction guidelines titled as such. It is the moderator’s choice how they wish deliver the included information i.e. by radio, email, etc. No script was developed. Also included in the scenarios are links to documents and forms that may be presented to a unit officer by the EMS Duty Officer if they were to be one of the group leaders. The intent of using these real documents and forms is to present the opportunity for the unit officers to be exposed to the documents and forms in training before they are expected to use them at an actual event.
This is a remote training session with three to four of your officers. The scenario also requires an officer to be in command. It is your choice if
you will be in command of the event or if you wish one of your officers to be ‘command'. The remaining officers will be a supervisor for one of the following groups:
Triage
Transport
Treatment
The officers will need to be at a computer terminal and have a radio available. Please contact B/C Baltrosky to secure a talkgroup for the training. Included are links to documents for you to email to your officers as the training unfolds.
Goals:
Utilize the task list to evaluate the participants in the events. In addition to the benchmarks, each event has individual milestones that should be reached.
Task list link:
This document will provide you with the framework to facilitate the training. There are specific interactions that you should have with your unit officers – these interactions are included in the document. Feel free to add or remove information at your will.
Type:
Shooting – ALS2
Address:
Pick an office park in your first due to add authenticity
Dispatched units:
3 or 4 of your primary units – two must be Paramedic Engines, as they are dispatched on the EMS task force. Add 5 transport units to the call – these units are available for transport and they will ghost units unless you wish to verbalize them checking on the scene on the radio.
Note: there is a similar event in another battalion, and there are no other units available for dispatch.
Comments:
Police are on the scene. The scene is safe – the threat has been neutralized. There are multiple shooting victims.
Goals:
- Maintain communication between supervisors and command
- Proper distribution of patients between trauma centers
Milestones:
- Establish command
- Designate supervisors for
- Triage
- Transport
- Treatment
Patient information:
- Patients have been assembled in a casualty collection point
- Total Patients: 7
- Acuity
- 2 Deceased
- 3 Immediate
- 1 Delayed
- 1 Minor
- Acuity
Transport units:
Transport units in a MCI should be moving patients. There are no additional transport units available in the county. If command or one of the group supervisors dedicates a transport unit to a task other than that of transporting a patient, do not allow the unit to be used for transport without adding a significant delay to its availability.
Triage Group Supervisor
Interaction:
The Triage Group Supervisor should utilize their crew to perform the triage. The supervisor should receive this return from their crew:
- 7 Patients total – all traumas
- Acuity
- 2 Deceased
- 3 Immediate
- 2 Pediatric
- 1 Adult
- 1 Delayed
- Adult
- 1 Minor
- Pediatric
- Acuity
Transport Group Supervisor
Interaction:
The Transport Group Supervisor will need to obtain hospital bed availability and track the patients as they are moved to the hospitals.
This is the bed availability:
- Baltimore Shock Trauma
- 4 Immediate
- 2 Delayed
- 0 Minor
- Children’s DC
- 3 Immediate
- 4 Delayed
- 0 Minor
- Suburban Trauma
- 1 Immediate
- 1 Delayed
- 1 Minor
- MedStar Trauma
- 2 Immediate
- 2 Delayed
- 0 Minor
The Transport Group Supervisor is responsible for managing the ambulance staging area. These are the 5 ambulances dispatched in the EMS task force. There are no additional transport units available.
The Transport Group Supervisor should coordinate with the treatment group supervisor and move the patients out to the appropriate hospitals as soon as the patients are ready. They should also document the amount of patients transported to each hospital and the destination for each patient.
The Transport Group Supervisor and the Treatment Group Supervisor should be communicating to each other via the radio.
The Transport Group Supervisor, or their designee, is the only person that shall communicate with the hospitals.
Treatment Group Supervisor
Interaction:
The Treatment Group Supervisor will utilize the crew of their unit to treat the patients as they arrive in treatment area.
The crew from the triage group should be reassigned to work under the Treatment Group Supervisor after triage is complete. This manpower unit will be the victim carriers needed to assemble the patients in the treatment area. The treatment area should be in the cold zone - away from the casualty collection point.
The facilitator should tell the treatment group supervisor when they have patients in the treatment area and when the victims are ready for transport. The immediates should be moved out first, followed by delayed, and then minor. Randomize the severity of the victims that are arriving and ready for transport so that the supervisor may execute the proper decisions.
MCI Drill for Unit & Battalion Chief Officers
Carbon Monoxide Incident
Type:
Hazmat/Full
Address:
Pick a building in your first due to add authenticity
Dispatched units:
3 or 4 of your primary units – at least 2 paramedic engines. The units you are working with have been dispatched in an EMS task force with additional manpower piece(s). Add 5 transport units to the call – these units are available for transport and they will ghost units unless you wish to verbalize them checking on the scene on the radio.
Note: there is a multi-alarm fire in another battalion, and there are no other units available for dispatch.
Comments:
Command is established. These units have been added to assist with patient treatment and transport
Goals:
- Maintain communication between unit leaders and the EMS Group Supervisor
- Reds must be transported to hyperbaric medicine
- Yellows and greens need to be evaluated and distributed to the correct hospitals
Milestones:
- Establish EMS Group (by you or one of your officers)
- Designate leaders for the
- Triage Unit
- Transport Unit
- Treatment Unit
Patient information:
- Patients have been assembled in a collection point
- Total Patients: 7
- Acuity
- 2 Red
- 1 Yellow
- 4 Green
- Acuity
Transport units:
Transport units in a MCI should be moving patients. There are no additional transport units available in the county. If one of the unit leaders or the EMS group supervisor dedicates a transport unit to a task other than that of transporting a patient, do not allow the unit to be used for transport without adding a significant delay to the its availability.
Send your officers emails with links to these documents or the documents in attachments. Stagger the unit arrivals as you see fit.
The unit that is the EMS Group Supervisor should receive this document:
https://www.dropbox.com/s/bm95w2g3ogl86ji/local_command_charts.pdf?dl=0
The triage unit leader should receive this document:
https://www.dropbox.com/s/bxfhikgi8ueliau/MC%20Triage%20Unit%20Leader%20%231.pdf?dl=0
The transport unit leader should receive these documents:
https://www.dropbox.com/s/rx3od22a70xbubl/Transportation%20Supervisor%20Checklist.pdf?dl=0
https://www.dropbox.com/s/bse56qlh3whnkz8/MC%20Transportation%20Group%20Supervisor%234.pdf?dl=0
https://www.dropbox.com/s/eluf9uwmalm2sac/MIEMSS%20Transportation%20Disposition%20Officer%20Log.doc?dl=0
https://www.dropbox.com/s/72pl5fn7ef86l3e/MC%20Medcomm%20Worksheet%20%233.pdf?dl=0
The treatment unit leader should receive these documents:
https://www.dropbox.com/s/khkuqna2ophjp02/Treatment%20Supervisor%20Checklist.pdf?dl=0
https://www.dropbox.com/s/el9roh4zuwtmw2h/MC%20Triage%20Unit%20Leader%20%231.pdf?dl=0
https://www.dropbox.com/s/zw4whrddl7cxjjj/MIEMSS%20Patient%20Tracking%20form.xls?dl=0
Type:
Shooting – ALS2
Address:
Pick an office park in your first due to add authenticity
Dispatched units:
3 or 4 of your primary units – two must be Paramedic Engines, as they are dispatched on the EMS task force. Add 5 transport units to the call – these units are available for transport and they will ghost units unless you wish to verbalize them checking on the scene on the radio.
Note: there is a similar event in another battalion, and there are no other units available for dispatch.
Comments:
Police are on the scene. The scene is safe – the threat has been neutralized. There are multiple shooting victims.
Goals:
- Maintain communication between supervisors and command
- Proper distribution of patients between trauma centers
Milestones:
- Establish command
- Designate supervisors for
- Triage
- Transport
- Treatment
Patient information:
- Patients have been assembled in a casualty collection point
- Total Patients: 7
- Acuity
- 2 Deceased
- 3 Immediate
- 1 Delayed
- 1 Minor
- Acuity
Transport units:
Transport units in a MCI should be moving patients. There are no additional transport units available in the county. If command or one of the group supervisors dedicates a transport unit to a task other than that of transporting a patient, do not allow the unit to be used for transport without adding a significant delay to its availability.